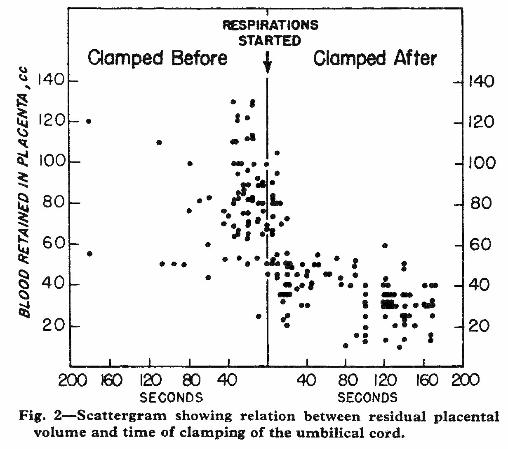
Plot of blood left in the placenta
when the cord was clamped
before onset of respiration (left)
or after (right).
From Redmond et al. (1965)
when the cord was clamped
before onset of respiration (left)
or after (right).
From Redmond et al. (1965)
Transfer of blood from placenta to lungs
Redmond et al. (1965) measured residual placental
blood as an estimate of placental transfusion before
and after onset of respiration. In 55 infants, the cord
was clamped before onset of respiration, and in 97
after the onset of respiration. The plot of residual
blood to onset of respiration (right & below) from the
paper by Redmond et al. shows a dramatic drop in
residual blood in cases where the cord was clamped
after onset of respiration. Their own explanation of
the data cannot be improved upon:
observed by Dawes et al. (1953) in lambs, but
pointed out that Dawes et al. removed placental
circulation by clamping the cord in their experiments
[2]. Redmond et al. did not cite the work of Jäykkä
(1954) a year earlier showing that fluid filling the
capillaries surrounding the alveoli would cause them
to open [3].
Beyond mechanical filling of the capillaries, the
biochemistry of hemoglobin needs to be considered.
Filling of the capillaries with blood brings hemoglobin
to the alveoli laden with carbon dioxide, which may
need to be exhaled before oxygen is taken up.
Stemberra et al. (1963) provided evidence that
placental circulation continues during the first 2
minutes after birth, whether or not respiration via the
lungs has begun [4]. Receipt of oxygen by newly
opened alveoli must be a first step. Sending blood
with progressively more oxygen back to the placenta
may be a signal for the placenta to begin constriction
of the umbilical arteries, as suggested by Spivack
(1946) [5].
Placental respiration continues during the 2 minutes
of continuing placental circulation after birth. As
pointed out by White (1773) the changes in
circulation that take place following birth cannot be
brought about in one instant of time, and certainly not
at the will of a bystander with a clamp.
Redmond et al. (1965) measured residual placental
blood as an estimate of placental transfusion before
and after onset of respiration. In 55 infants, the cord
was clamped before onset of respiration, and in 97
after the onset of respiration. The plot of residual
blood to onset of respiration (right & below) from the
paper by Redmond et al. shows a dramatic drop in
residual blood in cases where the cord was clamped
after onset of respiration. Their own explanation of
the data cannot be improved upon:
- "Our data, obtained from normal uncomplicated
pregnancies, clearly demonstrated that a
placental transfusion is an inevitable
physiological consequence of initial pulmonary
expansion, over which obstetricians and
paediatricians have little, if any, control.
...In infants who breathed before cord clamping,
the difference in residual placental volume
between those whose cords were clamped one
minute after delivery and those whose cords
were clamped three minutes or more after
delivery was small...
...Had we defined early clamping and late
clamping simply in relation to time of delivery, a
number of babies whose cords were clamped
within one minute would have been described as
'clamped early' (and by implication to have been
deprived of placental blood); whereas placental
transfusion had in fact already occurred..."
"...In a survey (Redmond and Ingall 1964) of 100
random deliveries * performed by 32
obstetricians in a private maternity hospital, the
following figures were of interest. The time from
delivery of the chin to delivery of the entire body
averaged thirty-three seconds, to clamping
fifty-nine seconds, and to first gasp thirty-eight
seconds. Almost two-thirds of these babies
gasped during delivery of the body and could
have received a placental transfusion. The
other third had their cords ligated before the first
gasp and were probably deprived of their
placental blood. More than 90% of these babies
had their cords clamped within a minute of
delivery of the body (usual definition of early
clamping). Although objective evidence was not
obtained, we suggest that most of the babies
could have received their placental blood before
clamping if breathing started before ligation of
the cord. The tendency for some obstetricians
to deliver the head, aspirate the nose and
mouth, and slowly extract the remainder of the
baby probably aids the transmission of placental
blood to the infant." [1, p284]
"The present evidence shows a definite relation
between onset of respiration and occurrence of
a placental transfusion, but the mechanism is
not clear." [1, p285]
observed by Dawes et al. (1953) in lambs, but
pointed out that Dawes et al. removed placental
circulation by clamping the cord in their experiments
[2]. Redmond et al. did not cite the work of Jäykkä
(1954) a year earlier showing that fluid filling the
capillaries surrounding the alveoli would cause them
to open [3].
Beyond mechanical filling of the capillaries, the
biochemistry of hemoglobin needs to be considered.
Filling of the capillaries with blood brings hemoglobin
to the alveoli laden with carbon dioxide, which may
need to be exhaled before oxygen is taken up.
Stemberra et al. (1963) provided evidence that
placental circulation continues during the first 2
minutes after birth, whether or not respiration via the
lungs has begun [4]. Receipt of oxygen by newly
opened alveoli must be a first step. Sending blood
with progressively more oxygen back to the placenta
may be a signal for the placenta to begin constriction
of the umbilical arteries, as suggested by Spivack
(1946) [5].
Placental respiration continues during the 2 minutes
of continuing placental circulation after birth. As
pointed out by White (1773) the changes in
circulation that take place following birth cannot be
brought about in one instant of time, and certainly not
at the will of a bystander with a clamp.
- Redmond A et al. (1965)
Relation of onset of
respiration to placental
transfusion. - Dawes GS et al. (1953)
Changes in the lungs of the
newborn lamb. - Jäykkä S (1954) A new
theory concerning the
mechanism of the initiation
of respiration in the
newborn; a preliminary
report. - Stembera ZK et al. (1965)
Umbilical blood flow in
healthy newborn infants
during the first minutes after
birth. - Spivack M (1946) The
anatomic peculiarities of the
human umbilical cord and
their clinical significance. - White C (1773) A Treatise on
the Management of Pregnant
and Lying-In Women.
- Redmond A, Isana S, Ingall D. Relation of onset of respiration to placental
transfusion. Lancet. 1965 Feb 6;1:283-5. - Dawes GS Mott JC, Widdicombe JG, Wyatt DG. Changes in the lungs of
the newborn lamb J. Physiol. 1953 Jul; 121:141-162 - Jäykkä S. A new theory concerning the mechanism of the initiation of
respiration in the newborn; a preliminary report. Acta Paediatr. 1954 Sep;
43(5):399-410. - Stembera ZK, Hodr J, Janda J. Umbilical blood flow in healthy newborn
infants during the first minutes after birth. Am J Obstet Gynecol. 1965 Feb
15;91:568-74. - Spivack M. The anatomic peculiarities of the human umbilical cord and
their clinical significance. Am J Obstet Gynecol 1946 Sep; 52(3):387-401. - White C (1773) A Treatise on the Management of Pregnant and Lying-In
Women. Canton, MA: Science History Publications, 1987, p 45 Available
from: http://www.shpusa.com/bkindex.html
Plot of blood left in the placenta when the cord was clamped before onset of
respiration (left) or after (right). From Redmond et al. (1965)
respiration (left) or after (right). From Redmond et al. (1965)