A Parting Gift
An editorial in the Lancet for January 28, 1967
introduced a paper by Kjeldsen and Pedersen
(1967) on the respiratory-distress syndrome [1, 2],
and opened with the following comments and
questions:
The second question is odd. Blood in the placenta
should be compared to blood circulating in the lungs
after a baby begins breathing. The placenta is the
prenatal organ of respiration. The blood rightfully
belongs to the infant, of course. There is no need
for blood in the placenta once respiratory function
has been taken over by the lungs.
Continuing pulsations in the umbilical cord after birth
are from the infant's heart continuing to pump blood
to the placenta as the lungs begin to expand with the
first few breaths. When pulsations cease, little blood
remains in the placenta. Unless interrupted by
premature clamping of the cord, placental blood
continues to deliver oxygen to the baby as it is
transferred to the expanding circulatory system of
the lungs [5, 6]
The editorial writers summarized and compared the
research of Usher et al. (1963) and Redmond et al.
Usher et al. used a radioactive tracer to measure the
blood volume of newborn infants [4]. Redmond
measured residual blood in the placenta [5].
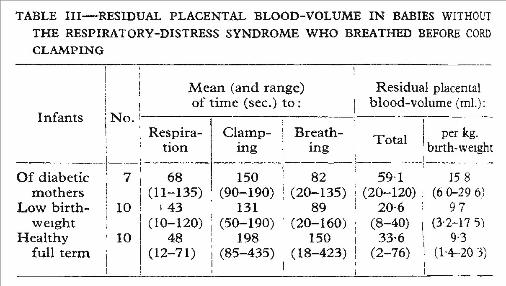
introduced and discussed. Kjeldsen and Pedersen
used the method of Redmond et al. [5] to measure
residual placental volume in infants of diabetic
mothers, low birth weight infants, and normal-term
infants. Residual volume for infants of diabetic
mothers was found to be almost double that of the
normal-term infants. Infants of diabetic mothers
were also slower to begin breathing.
The larger residual placental blood appears to be
related to greater fetal blood volume in diabetic
preganancies. Furhter research on maternal
diabetes has revealed that enlargement of the fetal
heart and differences in fetal-placental blood flow
during pregnancy are common. Up to 8 percent of
children of diabetic mothers have persistent heart
defects [7].
In addition to finding greater residual placental blood
in maternal diabetes, Kjeldsen and Pedersen
confirmed the finding of Redmond et al.:
This study included 26 infants of diabetic mothers
and 10 normal full-term infants. Although large for
gestational age, the infants of diabetic mothers were
delivered after induction of labor about 3 weeks
before term. Thus 23 low birth-weight infants with
almost the same degree of prematurity were
included in this study.
Of the 23 low birth-weight infants, 13 developed the
respiratory distress syndrome (RDS) and 3 of these
died. Near-total pulmonary atelectasis was found at
necropsy in all 3 infants who died with RDS. The
average residual blood volume was larger in the low
birth-weight infants who developed RDS. Seven of
the 26 infants of diabetic mothers developed RDS,
which was not correlated with residual placental
blood, and all survived. In both groups incidence of
RDS was higher in infants who had not breathed
before the cord was clamped.
One of the infants of a diabetic mother died
unexpectedly at 4 days of age, and was found to
have congenital heart problem (coarctation of the
aorta).
The routine methods of delivery of the infants in this
research study are of interest:
cord occurred one minute or more after birth, except
in cases when resuscitation was needed. Residual
placental blood volume could therefore be reported
along with time to onset of respiration (and maximal
placental transfusion) before clamping of the cord.
See table III from Kjeldsen and Pedersen below.
The findings of Kjeldsen and Pedersen and
Redmond et al. would seem to suggest that allowing
placental transfusion following birth is more than a
parting gift. It should be viewed as a birth right.
An editorial in the Lancet for January 28, 1967
introduced a paper by Kjeldsen and Pedersen
(1967) on the respiratory-distress syndrome [1, 2],
and opened with the following comments and
questions:
- "In the age of astronauts it is odd that we are still
undecided about so small but fundamental a
detail as when-or, for that matter, how-best to
ligate the umbilical cord. The difficulty stems
from the fact that a relatively large volume of
blood can be transferred to the infant within a
few seconds of birth and that, rarely, such
plethora may embarrass cerebral blood-flow
and lead to convulsions and unconsciousness.
[3]. The normal baby at term receives a
placental transfusion of as much as 60% of his
blood-volume when clamping of the cord is
delayed for five minutes [4]. Is this a
physiological necessity, and, if so, what are the
consequences when the infant is deprived of it?
Does this large volume of blood rightfully belong
to the infant or to his placenta? And how is this
massive transfusion related to the onset of
respiration and circulatory adaptation at birth?"
[1, p201]
The second question is odd. Blood in the placenta
should be compared to blood circulating in the lungs
after a baby begins breathing. The placenta is the
prenatal organ of respiration. The blood rightfully
belongs to the infant, of course. There is no need
for blood in the placenta once respiratory function
has been taken over by the lungs.
Continuing pulsations in the umbilical cord after birth
are from the infant's heart continuing to pump blood
to the placenta as the lungs begin to expand with the
first few breaths. When pulsations cease, little blood
remains in the placenta. Unless interrupted by
premature clamping of the cord, placental blood
continues to deliver oxygen to the baby as it is
transferred to the expanding circulatory system of
the lungs [5, 6]
The editorial writers summarized and compared the
research of Usher et al. (1963) and Redmond et al.
Usher et al. used a radioactive tracer to measure the
blood volume of newborn infants [4]. Redmond
measured residual blood in the placenta [5].
- "USHER et al. [4], using [131]I-albumin, studied
the blood volume changes of normal-term
babies. A 3500 g. infant had an average blood-
volume of 275 ml., which was augmented by a
transfusion of 160 ml. from the placenta if the
cord was not occluded for five minutes. Of this,
a quarter was transferred in fifteen seconds and
half in the first minute; and most of the
transfused blood had left the circulation after
four hours as a result of plasma shifts. By the
third day, when the blood-volume had become
stable, the average value for infants who had
received no transfusion was 82 ml. per kg.
(venous haematocrit 44%) as against 93 ml. per
kg. (haematocrit 60%) in those who had.
REDMOND et a1.[5] measured the residual
placental blood-volumes at 191 uncomplicated
vertex deliveries by the simple expedient of
allowing the placenta to drain into a graduated
cylinder from a height of 18 inches for twenty
minutes. The residual placental volume was
assumed to be indirectly proportional to the
volume transfused, and was shown to depend
not so much on the time of clamping of the cord
as on whether it was clamped before or after
the onset of respiration. The volume of blood
left in the placenta averaged 40 ml. when the
cord was clamped after the onset of respiration
and 85 ml. when it was clamped before. Thus, it
seems that a transfusion of blood normally
takes place within seconds of birth and that
approximately 45 ml. of this volume may be
accommodated in the pulmonary circulation." [1,
p201]
introduced and discussed. Kjeldsen and Pedersen
used the method of Redmond et al. [5] to measure
residual placental volume in infants of diabetic
mothers, low birth weight infants, and normal-term
infants. Residual volume for infants of diabetic
mothers was found to be almost double that of the
normal-term infants. Infants of diabetic mothers
were also slower to begin breathing.
The larger residual placental blood appears to be
related to greater fetal blood volume in diabetic
preganancies. Furhter research on maternal
diabetes has revealed that enlargement of the fetal
heart and differences in fetal-placental blood flow
during pregnancy are common. Up to 8 percent of
children of diabetic mothers have persistent heart
defects [7].
In addition to finding greater residual placental blood
in maternal diabetes, Kjeldsen and Pedersen
confirmed the finding of Redmond et al.:
- "We have confirmed the correlation of the
residual placental blood-volume with the onset
of respiration, before and after cord clamping,
demonstrated by Redmond et al. (1965). In DM
and LBW infants the residual volume was
smaller when the infant breathed before the
cord was tied." [2, p183]
This study included 26 infants of diabetic mothers
and 10 normal full-term infants. Although large for
gestational age, the infants of diabetic mothers were
delivered after induction of labor about 3 weeks
before term. Thus 23 low birth-weight infants with
almost the same degree of prematurity were
included in this study.
Of the 23 low birth-weight infants, 13 developed the
respiratory distress syndrome (RDS) and 3 of these
died. Near-total pulmonary atelectasis was found at
necropsy in all 3 infants who died with RDS. The
average residual blood volume was larger in the low
birth-weight infants who developed RDS. Seven of
the 26 infants of diabetic mothers developed RDS,
which was not correlated with residual placental
blood, and all survived. In both groups incidence of
RDS was higher in infants who had not breathed
before the cord was clamped.
One of the infants of a diabetic mother died
unexpectedly at 4 days of age, and was found to
have congenital heart problem (coarctation of the
aorta).
The routine methods of delivery of the infants in this
research study are of interest:
- "The routine methods of the department were
observed. At the moment of delivery of the
anterior shoulder methylergometrine maleate 0-
2 mg. was given intramuscularly to all mothers.
If the infant had been delivered by the vaginal
route he was placed in the delivery bed below
the vulva. Furthermore, if delivery was by
caesarean section oxytocin 10 I.U. was injected
into the uterine muscle at the moment of
delivery, and the infant was held by his feet with
his head down, lower than placenta if possible.
Clamping of the cord 60 seconds or more after
delivery was our standard procedure, but the
cord was not stripped. Early clamping was
applied routinely whenever urgent resuscitation
was found necessary
By caesarean section, delivery was
intentionally slow in head presentations to mimic
the squeezing of thorax seen in normal vaginal
delivery (Karlberg 1960, Karlberg et al. 1962).
We have no standard routine for timing of
clamping in delivery by section." [2, p181]
cord occurred one minute or more after birth, except
in cases when resuscitation was needed. Residual
placental blood volume could therefore be reported
along with time to onset of respiration (and maximal
placental transfusion) before clamping of the cord.
See table III from Kjeldsen and Pedersen below.
The findings of Kjeldsen and Pedersen and
Redmond et al. would seem to suggest that allowing
placental transfusion following birth is more than a
parting gift. It should be viewed as a birth right.
- Lancet editorial (1967) [No
authors listed] A parting gift. - Kjeldsen J, Pedersen J
(1967) Relation of residual
placental blood-volume to
onset of respiration and the
respiratory-distress
syndrome in infants of
diabetic and non-diabetic
mothers. - Wood JL (1959) Plethora in
the newborn infant
associated with cyanosis
and convulsions: A review of
postnatal erythropoiesis. - Usher R et al. (1963) The
blood volume of the newborn
infant and placental
transfusion. - Redmond A et al. (1965)
Relation of onset of
respiration to placental
transfusion. - Štembera ZK, et al. (1965)
Umbilical blood flow in
healthy newborn infants
during the first minutes after
birth. - Hornberger LK (2006)
Maternal diabetes and the
fetal heart.
- Anonymous editorial [No authors listed] A parting gift. Lancet. 1967 Jan 28;
1(7483):201-2 - Kjeldsen J, Pedersen J. Relation of residual placental blood-volume to
onset of respiration and the respiratory-distress syndrome in infants of
diabetic and non-diabetic mothers. Lancet. 1967 Jan 28;1(7483):180-4. - Wood JL. Plethora in the newborn infant associated with cyanosis and
convulsions: A review of postnatal erythropoiesis. Journal of Pediatrics
1959 Feb; 54(2):143-151. - Usher R, Shephard M, Lind J. The blood volume of the newborn infant and
placental transfusion. Acta Paediatr. 1963 Sep;52:497-512. - Redmond A, Isana S, Ingall D. Relation of onset of respiration to placental
transfusion. Lancet. 1965 Feb 6;1:283-5. - Štembera ZK, Hodr J, Janda J. Umbilical blood flow in healthy newborn
infants during the first minutes after birth. Am J Obstet Gynecol. 1965 Feb
15;91:568-74. - Hornberger LK. Maternal diabetes and the fetal heart. Heart. 2006 Aug;92
(8):1019-21.